

Why do women feel such shame about being seen to indulge, whether or not they are fat? Why do others take such glee in shaming them? Why does this extend even to non-indulgent foods?
I was recently at a social gathering of adults over the age of 25, the vast majority of whom hold PhDs and were academics. At this gathering, a male attendee speaking to a group of about seven people began to mock a pair of fat women he used to encounter who would walk together down the sidewalk briskly and clearly for exercise, and whom he would occasionally see end their walk at a fast food restaurant. He commented about the irony of this, and how much space they took up on the sidewalk which required him to get off the sidewalk to let them pass—as though this would not have been the case with two smaller women walking side by side—and connected this with their eating habits and fatness. Despite gentle pushback from myself and one other woman at the gathering, he doubled down on their rudeness and his shaming of them for eating at the fast food place despite the fact that he had no knowledge of their health other than their body size, no knowledge of what they ordered or ate at the fast food place, and was using them as an object of fun in an “amusing” party story. The raconteur fully expected everyone in his audience to share his attitude. And in many audiences, everyone would have.
This sort of shaming of fat people for eating is common. A “normal” sized man eating a hamburger with juices dripping down his chin and an expression of ecstasy may well be perceived as enjoying his food, but a larger man doing the same thing is likely to be perceived as a glutton.
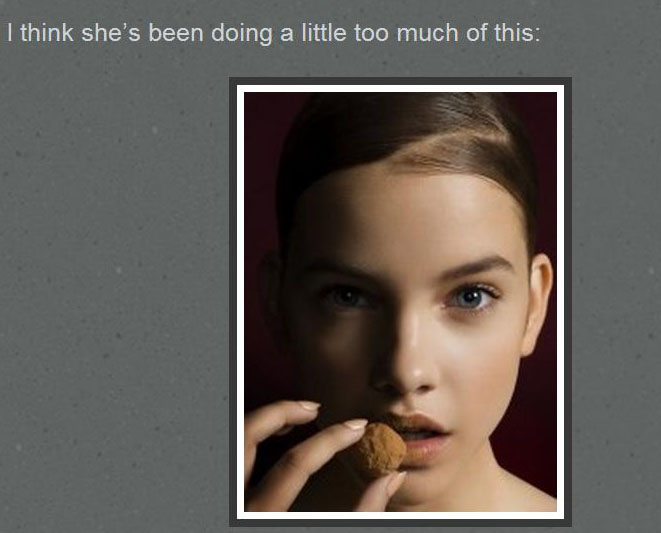
But it goes far beyond shaming of fat people. Even skinny people, especially women, are often made to feel shame for what they eat. Just consider the standard stock photo of women eating salad joyfully. Or this image of model Barbara Palvin with food near her mouth, presented on a “thinspo” (thinsporation) blog critiquing Palvin for gaining weight (though not enough that her thighs actually touch). The phrase which introduces it is from the blog’s author, and is the way she herself introduced this image.
The same blog also attacks Kate Upton for her curvy figure. For those who don’t follow such things, Upton was Sports Illustrated’s 2012 Swimsuit Issue Covergirl. On a page called “Kate Upton is Well-Marbled”, Upton is routinely called a “cow” and the author bemoans what the fashion industry is coming to when Upton is representing the profession:
Look, I’ll admit – I love In’n’Out as much as the next gurl, but it’s not supposed to be an everyday thing, Kate! And we can be sure that Kate is the rare model who poses with food – and then actually devours it.

